This week’s case is a great example of a focal cemento-osseous dysplasia. Cemento-osseous dysplasia (COD) is a benign, reactive fibro-osseous lesion of the jaws. It goes through three stages of maturation, each with a distinct radiographic appearance. This case is from a cone beam CT, which really shows off the internal aspect of the lesion.
COD progresses through three stages of maturation, each with a distinct radiographic appearance:
- Stage 1 (Osteolytic) = Purely radiolucent. Early stage where the normal bone has been replaced by fibrous tissue. At this stage it can look very similar to a periapical inflammatory lesion — vitality testing is key.
- Stage 2 (Intermediate/Cementoblastic) = Mixed radiolucent and radiopaque. Calcified material (cementum-like and/or woven bone) begins to form within the fibrous tissue.
- Stage 3 (Mature) = Predominantly or completely radiopaque, often with a thin radiolucent rim at the periphery. The lesion has largely calcified and matured.
I’ll describe the radiographic appearance using my LESION acronym.
Focal Cemento-osseous Dysplasia
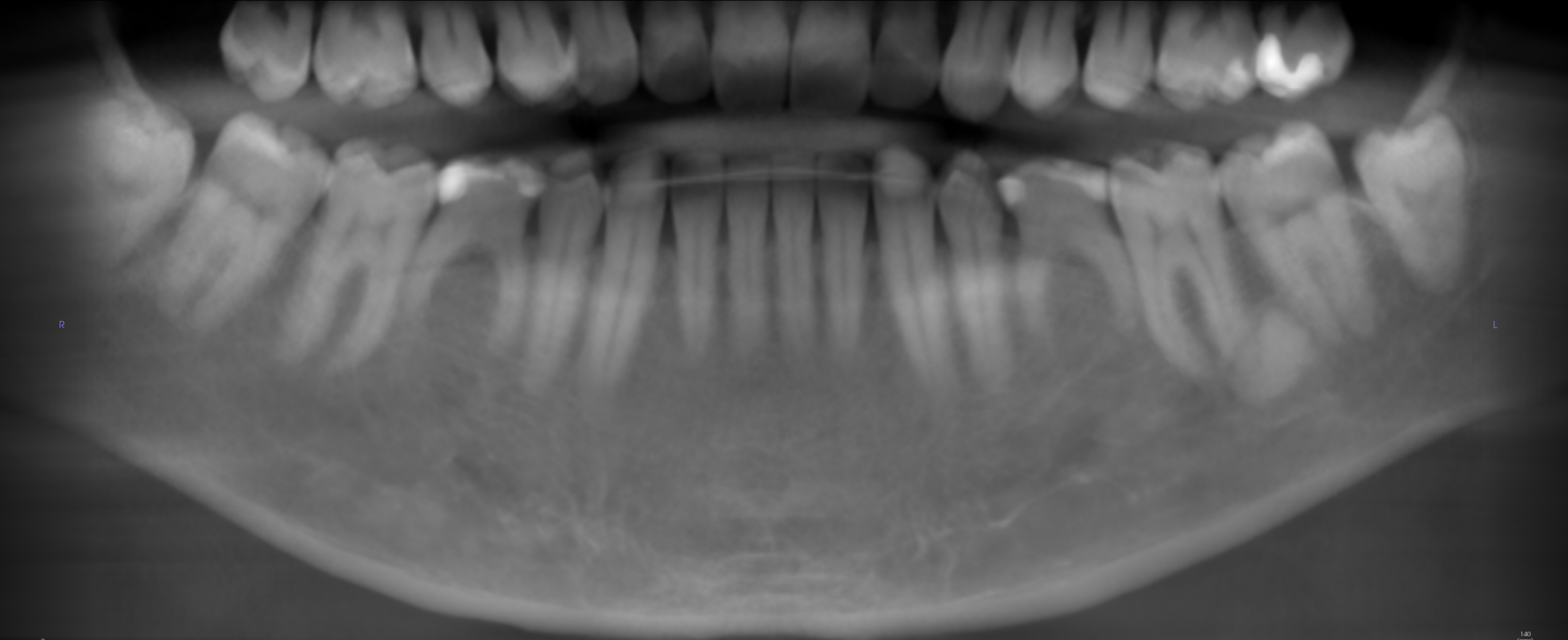
- Location = Posterior mandible (molar region); associated with the periapical region of a tooth.
- Edge = Well-defined; thin corticated border.
- Shape = No identifiable shape.
- Internal = Predominantly radiopaque — approaching Stage 3 (mature stage), though Stage 2 would also be accepted. The lesion is mostly calcified with minimal residual radiolucent areas.
- Other = Adjacent tooth/teeth appear vital (important distinguishing feature from periapical inflammatory disease); no root resorption noted; cortical plates appear intact with mild thinning.
- Number = Single (one quadrant involvement).

This is a case where CBCT is particularly helpful — the axial and cross-sectional slices allow you to appreciate the size, internal aspect, and extent of the lesion in all dimensions, which can be difficult to fully evaluate on a 2D pantomograph alone.
A key clinical pearl with cemento-osseous dysplasia: biopsy is not recommended for lesions with a classic radiographic presentation in a vital tooth, as it can introduce infection into an otherwise avascular lesion. Diagnosis is made based on the radiographic appearance and vitality testing. Periodic monitoring is the standard of care.

