Definition
Loss of bone due to inflammation at the apex or lateral aspect of a tooth root. The term encompasses periapical abscess, granuloma, and radicular/periapical cyst, as these cannot be reliably differentiated on a radiograph and require histopathologic examination for a definitive diagnosis. Sometimes referred to as apical rarefying osteitis or lateral rarefying osteitis based on location.
Etiology
Rarefying osteitis results from pulpal necrosis and the subsequent spread of infection or inflammatory mediators into the periapical tissues. Common causes of pulp death include deep caries, dental trauma, tooth fracture, or extensive restorative treatment. Bacteria and their byproducts from the necrotic pulp stimulate an immune response in the periapical bone, activating osteoclasts and resulting in bone resorption. Bone loss is not radiographically detectable until approximately 30–50% of mineral has been lost. Visible changes typically require 8–14 days to appear on a 2D radiograph (periapical radiograph or a pantomograph). A tooth may be necrotic without any visible bone loss on a radiograph.
Radiographic Features
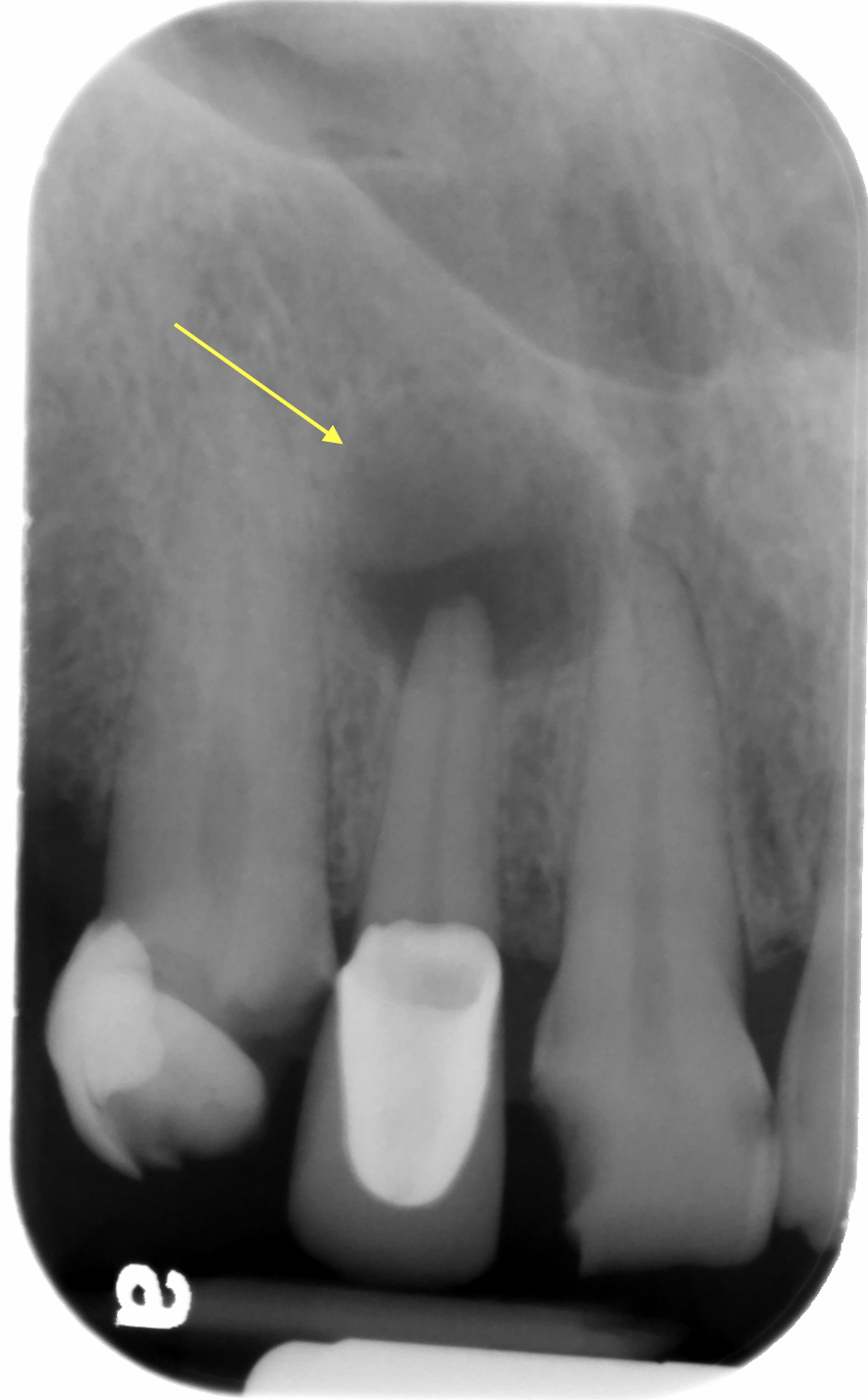
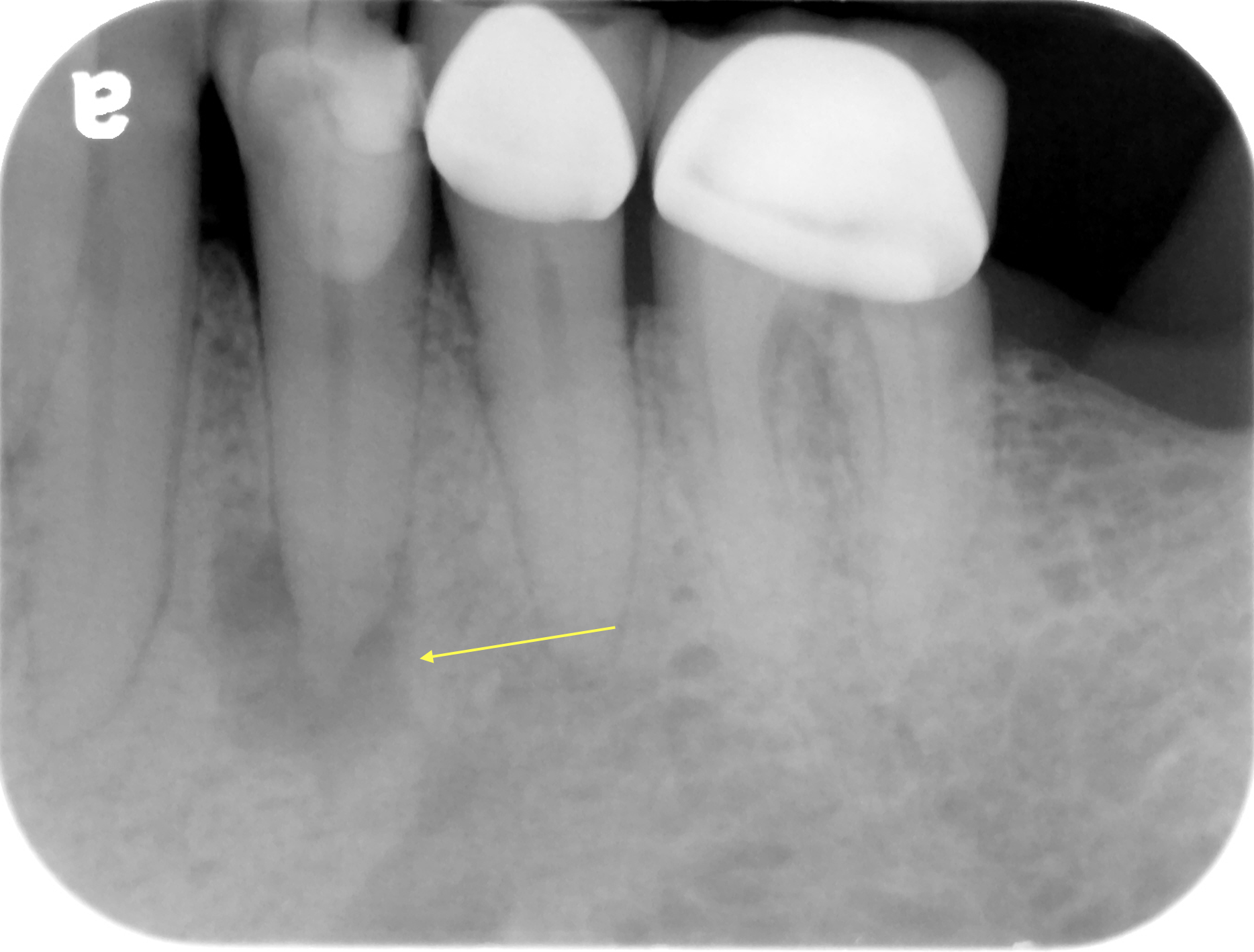
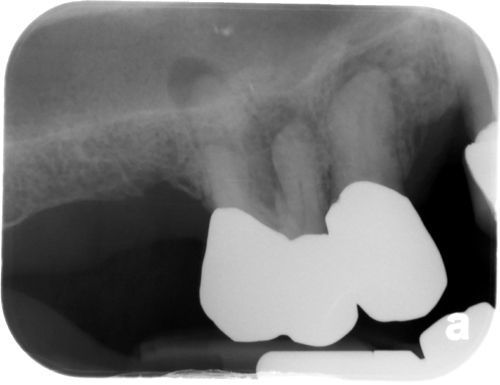
Location: Associated with a tooth, typically found at the apex. Can be found on the lateral aspect of a root when associated with a lateral canal.
Edge: Well-defined to Well-localized.
Shape: Round to ovoid, starts as a tear-drop shape at the apex with the lamina dura and periodontal ligament space pulling away from a tooth apex or source of inflammation.
Internal Structure: Radiolucent.
Other: Sometimes there is external root resorption of the associated tooth indicating granulomatous tissue.
Number: May be single or multiple.
Radiographic Examples
(click image to enlarge)



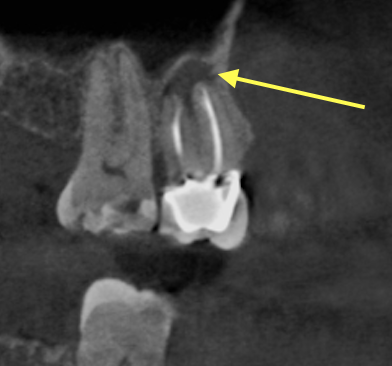
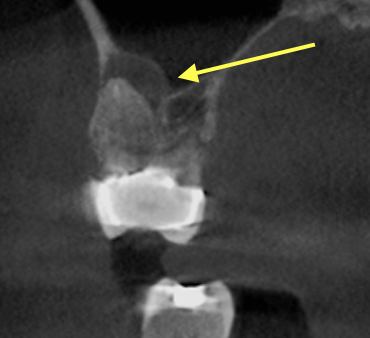
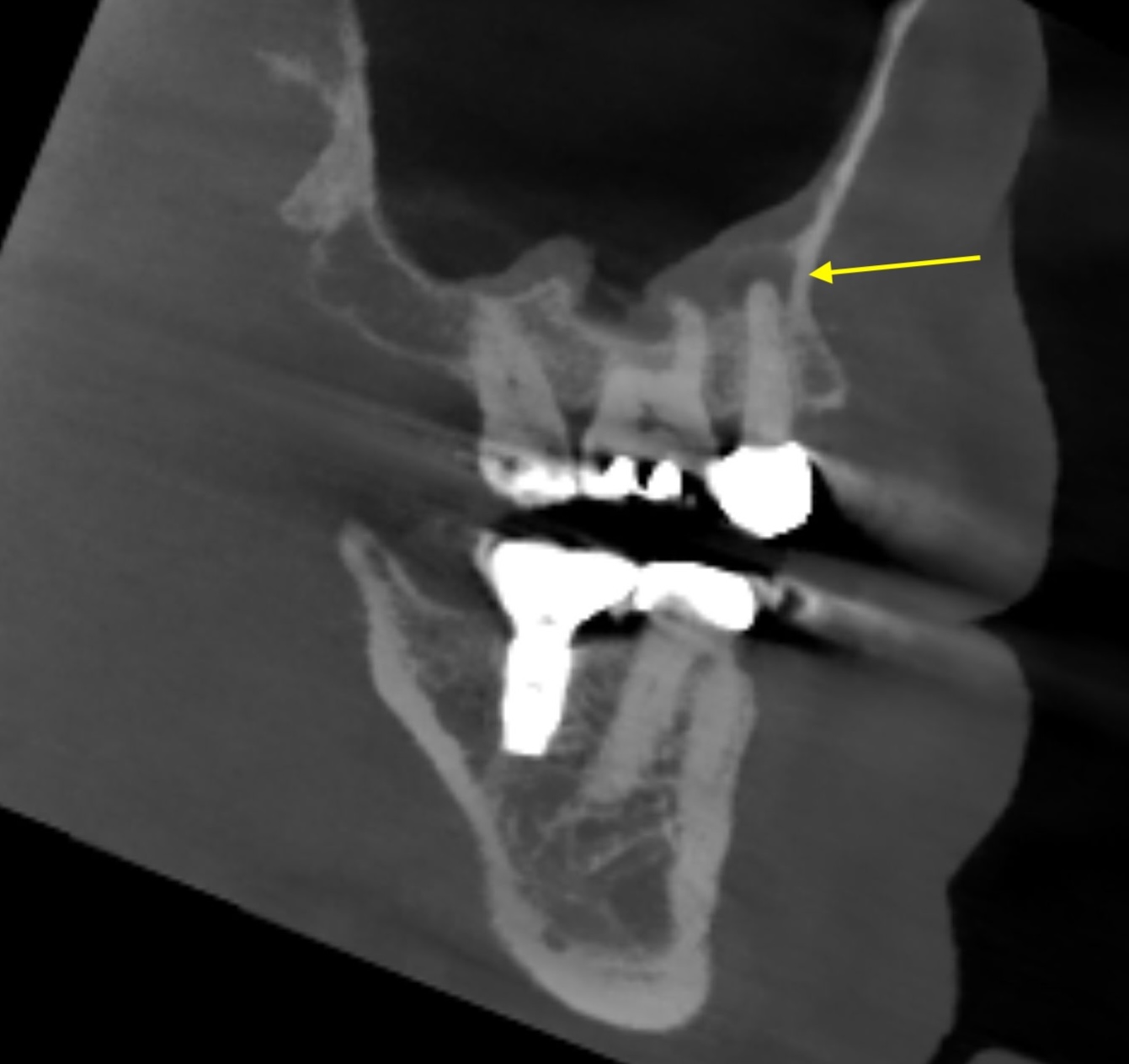
CBCT Slices


Clinical Significance
Rarefying osteitis indicates pulp necrosis and requires endodontic treatment (root canal therapy) or extraction. Because a tooth may be necrotic without visible radiographic change, clinical pulp vitality testing is essential and should not rely on radiographs alone. Early lesions may be subtle; comparison with prior radiographs is helpful for detecting change over time. Following successful endodontic treatment, bone regeneration should be observed radiographically over a period of 6–24 months.
Differential Interpretation
Periapical cemento-osseous dysplasia (early/lytic stage)
Early PCOD can appear as a periapical radiolucency closely mimicking rarefying osteitis. The key distinguishing feature is tooth vitality — the associated tooth is vital in PCOD. Pulp vitality testing is essential to differentiate these two entities.
Lateral periodontal cyst
A radiolucency on the lateral aspect of a root may resemble lateral rarefying osteitis. Lateral periodontal cysts are associated with vital teeth and typically display a well-defined, corticated border.
Normal anatomic landmarks
Structures such as the mental foramen, incisive foramen, or maxillary sinus may occasionally project over a root apex and mimic rarefying osteitis on a 2D radiograph. Repositioned radiographs or CBCT can help clarify.