Definition
Excessive deposition of cementum on the root surface of a tooth.
Etiology
The exact cause is often unknown (idiopathic), but several local and systemic conditions have been associated with hypercementosis:
- Chronic periapical inflammatory disease (e.g., chronic periapical periodontitis) — local irritation stimulates cementoblast activity
- Occlusal stress / hyperfunction — teeth subjected to excessive occlusal forces may develop hypercementosis as an adaptive response
- Paget’s disease of bone (osteitis deformans) — a systemic cause; typically produces irregular hypercementosis affecting multiple teeth
- Acromegaly — excess growth hormone can stimulate cementum deposition
- Hyperpituitarism
- Ankylosis (in some cases)
- Idiopathic — may occur in otherwise healthy individuals with no identifiable cause
Radiographic Features
Location: At the apex of the root; less commonly involves the entire root surface.
Edge: Well-defined.
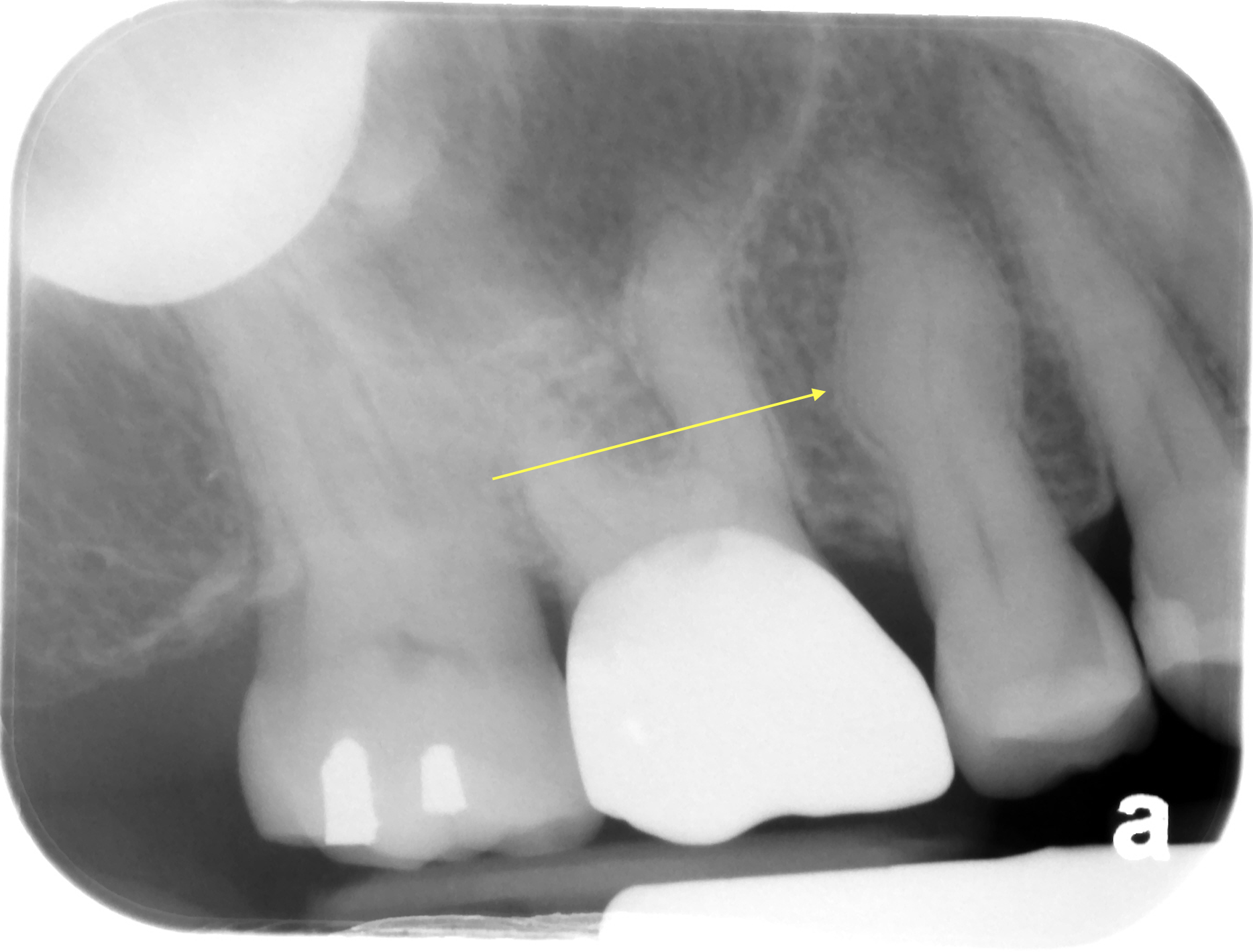
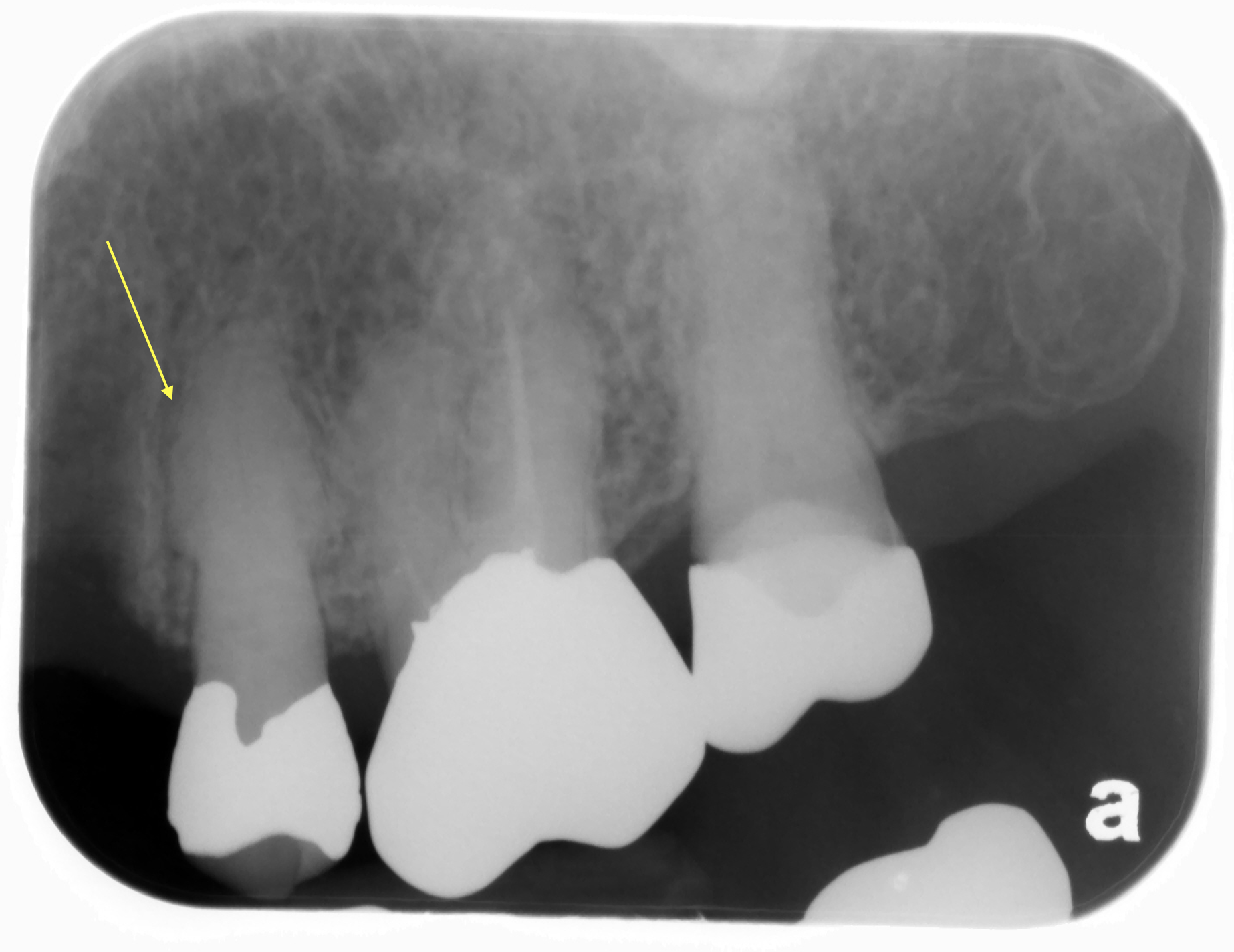
Shape: The root will have a bulbous, club-shaped, or nodular contour at the apex rather than tapering to a point as it normally would. The outline may be smooth or irregular. The irregular form is more commonly associated with systemic disease (e.g., Paget’s disease of bone).
Internal structure: Radiopaque. The additional cementum is less radiopaque than dentin and blends gradually with the existing root structure.
Other: The periodontal ligament (PDL) space will be continuous around the bulbous root — a thin radiolucent line visible at the apical enlargement confirms the radiopaque area is attached to the root, distinguishing hypercementosis from enostosis or focal idiopathic osteosclerosis (which lack a surrounding PDL space). The lamina dura is intact and continuous around the hypercementotic root.
Number: May be a single tooth or multiple teeth. Multifocal hypercementosis with an irregular outline should raise the suspicion of Paget’s disease of bone.
Radiographic Examples
(click image to enlarge)









CBCT slices




Clinical Significance
Hypercementosis is generally considered a benign finding and does not cause symptoms. However, its clinical importance lies in two areas:
- Extraction difficulty: Teeth with hypercementosis — particularly those with a bulbous or irregular root morphology — can be significantly more difficult to extract. The enlarged root may not pass through the bony socket without bone removal or tooth sectioning. Clinicians should anticipate this when treatment planning extractions.
- Recognition and accurate diagnosis: It is important to correctly identify hypercementosis radiographically and distinguish it from other apical pathoses (see Differential Interpretation below). Because the tooth is typically vital and non-tender, a misdiagnosis could lead to unnecessary endodontic treatment or other intervention.
Differential Interpretation
Based purely on imaging findings, the following should be considered when evaluating a radiopaque apical finding:
Cementoblastoma
A true neoplasm of cementoblasts. Appears as a large, well-defined radiopaque mass fused to the root apex, often with a radiolucent rim. The affected root may be resorbed into the mass. Unlike hypercementosis, the PDL space is not preserved around the mass. Cementoblastoma is typically associated with a vital tooth and may cause pain and expansion.
Enostosis (Bone Island) / Focal Idiopathic Osteosclerosis
Both are focal sclerotic bone changes that appear radiopaque near or at the root apex but are not attached to the root. The key radiographic distinction is the absence of a PDL space surrounding the finding — the sclerotic area blends into the surrounding bone without the thin radiolucent line seen in hypercementosis.
Periapical Cemento-Osseous Dysplasia (PCOD)
May have a mixed or radiopaque appearance depending on the stage of maturation. Early PCOD is radiolucent; as it matures, a central radiopaque mass forms surrounded by a radiolucent rim. Affects predominantly middle-aged women of African descent, with a predilection for the mandibular anterior region. Teeth are vital.
Sclerosing Osteitis
A localized area of sclerotic bone at the apex of a tooth with pulpal pathology. It represents a low-grade inflammatory reaction. Unlike hypercementosis, sclerosing osteitis is a bone response rather than a root change, and the normal root anatomy is preserved.
thank you 🙂 concise and full of usefull information
hi Dr G.
x ray belong to maxillary right canine, does not it look like enostosis? or focal osteosclerosis? I can not differentiate it.
it is a bit different from other examples to me.
thanks a tone.
If you look closely at maxillary right canine you will see a thin radiolucent line around the radiopaque area that is continuous with the periodontal ligament space of the canine indicating it is attached to the tooth root and not a hyperplasia of bone (enostosis or focal idiopathic osteosclerosis).
Hi Doc G!
The radiographs are great for understanding! Thank you so very much Doc!