This week I am going to show several examples of rarefying osteitis (sometimes referred to as apical rarefying osteitis when positioned at the apex). Rarefying osteitis is a term that means ‘loss of bone due to inflammation’. I use this term when describing a radiolucent area at the apex of a tooth that is non-vital. I typically do not specify between an abscess, cyst and/or granuloma as those are diagnosed histopathologically. Rarefying osteitis encompasses all three entities radiographically. This post I thought I would show some examples of each one individually and some signs you may see on a radiograph to help you determine which of the three it may be.
Periapical abscess
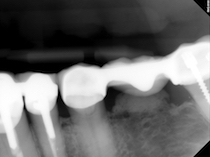
Sometimes an abscess will be associated with a sinus tract and this sinus tract may be evident as a radiolucent band/line extending from the apical rarefying osteitis to the crest of the alveolar ridge.

Note the radiolucent band on the distal aspect of the premolar. This was a sinus tract associated with an abscess.
Radicular / Periapical cyst
This will tend to be larger in size, closer to a 1 cm diameter.

Note the radiolucent area at the apices with a diameter of larger than 1 cm. This was a radicular / periapical cyst.
Periapical granuloma
A granuloma can be associated with external resorption of the associated tooth. Another thing to be aware of is that the size of a granuloma can also get quite large similar to a cyst. (I know confusing :S )

Note the external resorption of the apex of the central incisor and rarefying osteitis in the same location.
I realize that this may be a little confusing and that you won’t always have obvious signs as these. This is why I use the term rarefying osteitis indicating the loss of bone due to inflammation.
If you have any questions or are confused about the differences between the three entities, please let me know. You can also check out the pages on rarefying osteitis and radicular cyst for more information and radiographs.
Enjoy!

1st X-ray : recurrent caries i.r.t 47 mesial , root stump 46 endo-perio i.r.t 45 typical j shaped radiolucency
2nd xray distal composite filling i.r.t 22
1st – yes to root fragment of 46 (first molar) and J shape radiolucent area of 45 (second premolar). Not likely recurrent carious lesion on mesial of 47 (second molar).
2nd – yes.