Today I am going to give a little taste of a very hot topic currently involving cone beam CT and caries interpretation. While this debate is strongly divided, I would like to add a few thoughts and show what current research has found.
Current Research
The current research is a little all over the board. Here’s just a little sample of what you can find.
1) Rathore S et al. used extracted teeth with occlusal caries. They made intraoral radiographs and the Galileos (Sirona) cone beam CT unit on all the teeth. The presence or absence of caries was determined by histopathological slides after the teeth were imaged. The quick and short of this study showed that cone beam CT cannot be used for the sole purpose of occlusal caries interpretation.
2) Zhang ZL et al. used non-cavitated interproximal carious lesions on teeth and viewed them with a cone beam CT, analog film, and phosphor plate. They used a ProMax 3D (Planmeca) and a Kodak 9000 3D unit. They also determined the presence or absence of caries with histopathological slides after the teeth were imaged. They found that the detection of the caries on cone beam CT was similar to that on analog film and phosphor plates.
3) Park YS et al. performed a meta-analysis of all the research currently published on caries interpretation and cone beam CT. They found that cone beam CT is promising, yet traditional 2D radiographs are still the gold standard when interpreting for caries.
Thoughts
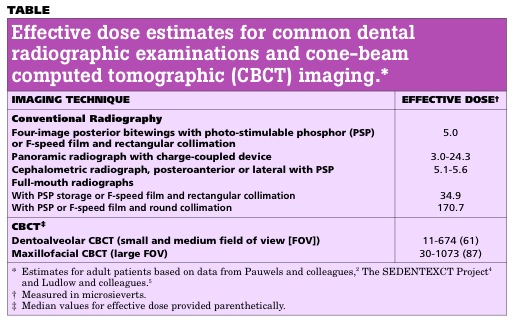
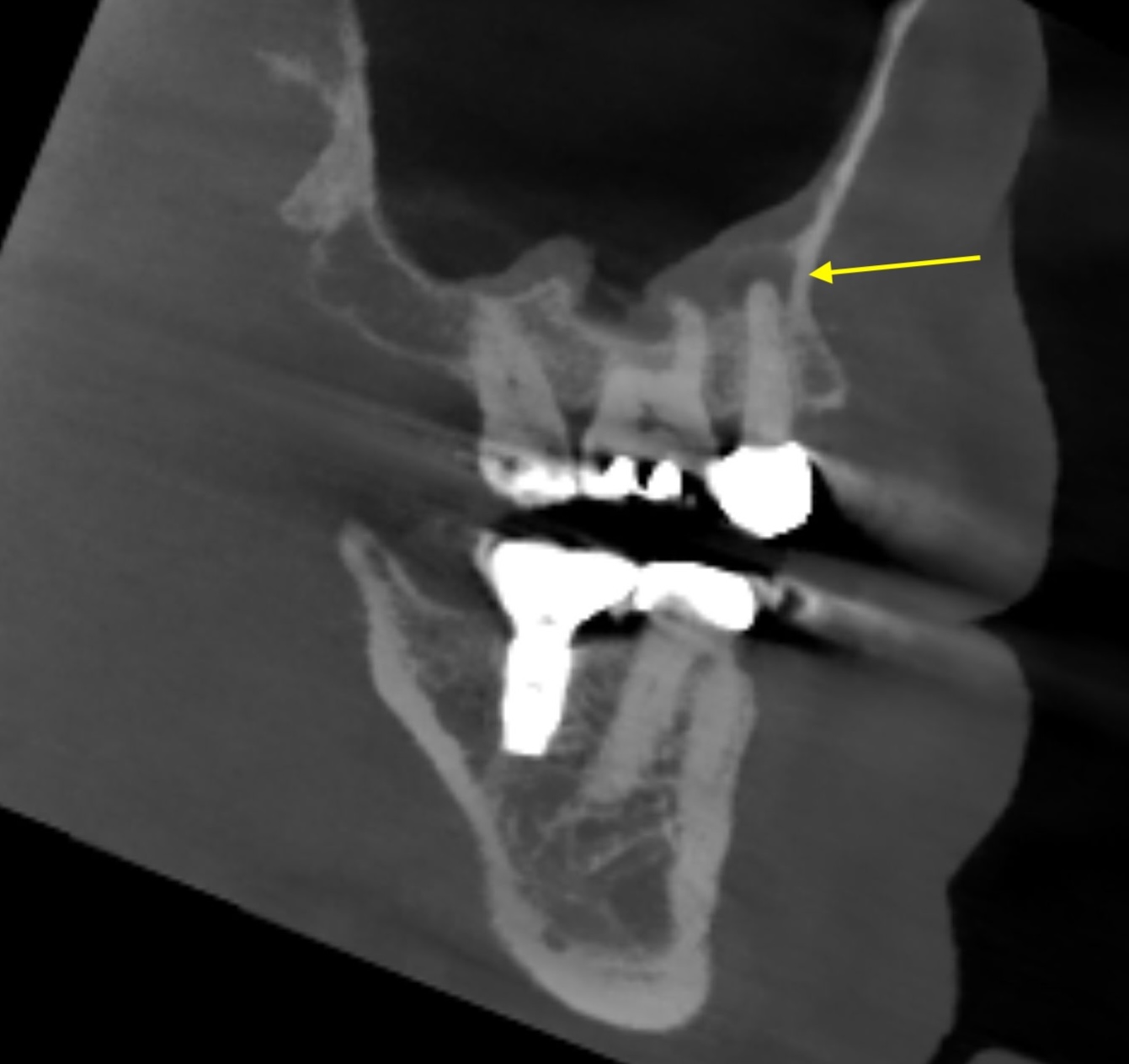
First when viewing a cone beam CT, the slice size must be taken into account. A larger slice size (0.4 mm) will have a lower spatial resolution and therefore be more difficult to use for caries interpretation. So IF you are going to use a cone beam CT to interpret for caries, try to use the smallest slice size possible. (Quick note – I am not advocating making a cone beam CT purely for caries interpretation, it would be secondary to another use, say implants, bony pathosis, etc. The amount of radiation exposure cannot be justified purely for caries interpretation when bitewings are still the gold standard and result in much less radiation exposure to the patient.) The biggest issue I have come across when using cone beam CT and caries interpretation is metal streaking artifact. While this artifact is less than with a traditional CT, it still is an artifact that obscures the coronal portion of the teeth. With this, caries interpretation is a mute point. Hence, I am not a fan nor do I use or advocate cone beam CT scans purely for caries interpretation. Below is an image showing metal artifact and how it obscures the adjacent teeth.

My final thought would be that cone beam CT is a great imaging modality for the maxillofacial region; HOWEVER, it still has a long ways to go before it can and will be used for caries interpretation solely (if ever due to the higher radiation dose to the patient).
Should you have any thoughts or observations you have made with caries interpretation and cone beam CT, I would greatly appreciate hearing them.
Thanks and enjoy!